
Table of contents
Do you have a “small” fang? Maybe it is a baby tooth.
The frequency of impacted upper canines is between 0.92% – 3.58%, being slightly more common if you are a girl. Most of the included canines (85%) are “asleep” in the roof of the mouth.

Orthodontists consider a tooth to be impacted when it remains completely or incompletely impacted in the oral mucosa for more than 2 years after it is due to erupt.
The teeth that are most frequently impacted are the last to erupt, that is, the so-called “wisdom teeth” that should appear at 18 years of age in the mouth and the upper canines that erupt at 12 years of age.
What might make you suspect that you have a crossed canine in the palate?
- AGE: the upper canine erupts at 13 years of age in boys and 12 in girls. Therefore, from the age of 15 in boys and 14 in girls without definitive canines, it is advisable to carry out a radiological study.
- Eruption time: once the milk tooth has been lost, the permanent tooth should erupt after approximately 4 months.
- PROBATION OF THE CANINE BULB: As it moves down the bone to its place, “bumps” can be felt under the lip on the gum, indicating the presence of the upper canines. This is palpable 2-3 years before eruption. (Between 9 and 12 years of age)
- COMPARISON WITH THE CONTRALATERAL: if there is more than 6 months difference between the eruption of one and the other it is advisable to take an orthopantomography.
And after suspecting, what do I do?
The first thing to do is to carry out a control orthopantomography to assess what is happening, it could be that there is a cyst that is preventing the eruption or extra teeth or that there is too much crowding and there is no room to erupt, for example.
In our clinic we carry out control orthopantomographies from the age of 8-9 years to assess the eruption of the canines and other pathologies. And we always carry out an orthopantomography at the first visit, regardless of your age.

Once confirmed it is necessary to carry out a study with a “TAC or dental scanner”. With this test we can see the teeth (even if they are inside the bone) in 3D, with the software we can make the bone disappear and see:
- the inclination
- the rotation
- the height
- the proximity to the midline of the mouth
- the relation to the roots of the other teeth…
In this way we will know exactly where it is located and what kind of movements have to be made to create a path to bring it down and put it in place between the other teeth.
Once it is located, can it always be put in place?
Most of the time they are in a favourable situation and can be put back in place between the other teeth.
Although not always, once the location has been studied (e.g. the higher it is, the more difficult it will be to lower it), the bite of all the teeth, the patient’s age, whether or not there are other teeth missing in that part of the mouth, etc., we can decide:
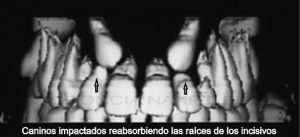
- Not to carry out any treatment, it is necessary to assess the risks involved in terms of resorption of nearby teeth (e.g. lateral incisors), cyst formation,…
- Surgical exposure and orthodontic traction there is no doubt that the best dental restoration is the natural teeth themselves. In order for the tooth to come out early, work well and have a great smile, it is necessary to plan in detail the route that the tooth will take and the movements of the neighbours that are going to support us in lowering the canine in its place.
- Extraction of the canine included, there are situations in which, after carefully assessing the position of the canine to be pulled (e.g. very high), the age of the patient (e.g. the older the patient, the greater the tendency to ankylosis, i.e. the tooth has fused with the bone and cannot move), the patient’s bite, etc… this is the best choice.
If you would like to make a free consultation to find out if you have a tusk inside the palate or not and what is the best treatment for your case, you can make a free appointment on 952 77 77 47.